

















Jeff Anderson's testimony begins at 40:00.
For many years, Americans have expressed a clear desire for real health-care reform. They want reform that would lower costs, increase choice, and improve the quality of care. Unfortunately, the Patient Protection and Affordable Care Act, commonly known as Obamacare, has taken us in the wrong direction in each of these areas.
Even more than that, Obamacare consolidates and centralizes power at the expense of Americans’ liberty. It severely restricts a free people’s ability to contract freely with one another. It mandates that, for the first time in more than 200 years of United States history, private American citizens must buy a product or service of the federal government’s choosing or else pay a penalty — what the law calls an “individual responsibility penalty” — for failure to comply with this command. A nation “conceived in Liberty” is living under a health-care law that is predicated on coercion.
What’s more, the Congressional Budget Office (CBO) now projects that Obamacare will cost American taxpayers $1.7 trillion over ten years for its insurance-coverage provisions alone — roughly double the $871 billion tab that was cited at the time of its passage through this body on Christmas Eve 2009.
At the same time, however, Americans are not particularly eager to return to the pre-Obamacare status quo. They have been waiting patiently — for six years now — for Obamacare opponents to unite around a free-market alternative that deals with costs, deals with coverage, and deals with the individual market without disrupting the employer-based market. The 2017 Project’s “Winning Alternative to Obamacare” would accomplish these goals, and the Supreme Court case of King v. Burwell provides a welcome opportunity to advance such an alternative, offer real reform, and give the American people what they want.
If the Court rules that, in states with federal exchanges, the Obama administration has been paying out subsidies in defiance of the law, Congress will have a prime opportunity to pass legislation that would do the following: Give the 37 affected states — as well as the 13 others — an off-ramp from Obamacare that would lower health costs, secure liberty, and ensure that anyone who wants to buy health insurance is able to do so. The result would be the effective repeal and replacement of Obamacare in up to 37 states — or even more, if some of the 13 states with their own exchanges chose to take the off-ramp as well.
This off-ramp should lead to a replacement that would fix what the federal government had already broken in our health-care system even before Obamacare was passed. For roughly 70 years, the government has provided a generous tax break for millions of Americans with employer-based health insurance, while millions of Americans who buy insurance on their own have been denied such a tax break. This is unfair, and it has undermined the individual market.
The “Winning Alternative to Obamacare” advanced by the 2017 Project — the organization I run — would address this unfairness in the tax code without touching the tax treatment of the typical American’s employer-based insurance. Those with employer-based insurance would continue to get their full tax break on insurance that costs up to $20,000 for a family or $8,000 for an individual, and anyone with a more expensive plan would still get the full tax break on that first $20,000 or $8,000.
An alternative advanced in the context of King v. Burwell would not have to address the employer-based market in any event, as that would be beyond the scope of the ruling. Such an alternative need only provide an overdue tax break for those in the individual market, in the form of a simple, non-income-tested, refundable tax credit.
Unlike Obamacare’s subsidies, which almost always go directly to insurance companies, these would be actual tax credits, going directly to individuals or families. For most Americans, they would come in the form of a tax cut.
Because the tax credits would not be income-based, they would be far simpler, reduce the IRS’s role, avoid disincentivizing work, avoid imposing a marriage penalty, and let every person or family quickly compute what they’d be getting. Perhaps most importantly, they would finally address the longstanding inequality in the tax code for all Americans.
The 2017 Project’s alternative would offer tax credits of $1,200 for those under the age of 35, $2,100 for those between 35 and 49, and $3,000 for those 50 and over — plus $900 per child. A family of four with 40-year-old parents would therefore get a tax credit of $6,000 to use for buying health insurance of their choice. If they shopped for value and found a policy for less, they could deposit the difference in a health savings account (HSA). The 2017 Project’s alternative would also offer a one-time, $1,000-per-person tax credit for having or opening an HSA, which would give a family of four another $4,000 in seed money to help cover out-of-pocket costs.
According to a Government Accountability Office report released on the eve of Obamacare’s implementation, tax credits in these amounts would be sufficient for healthy Americans to be able to buy insurance even if they paid no more than $15 a month of their own money toward the plans — except in five states, and people in those states could buy across state lines.
If Congress were to respond to a ruling against the Obama administration in King v. Burwell by offering such non-income-tested tax credits, it would benefit millions — perhaps tens of millions — of middle-class Americans who get nothing from Obamacare but the tab.
That’s because, for all of its expense and coercion, Obamacare did not solve the longstanding inequality in the tax code. Not only does Obamacare give subsidies to insurance companies, rather than tax cuts to Americans, but a wide swath of America has no access to the subsidies. According to the Kaiser Family Foundation calculator, the typical single woman who is 40 years old — or younger — and makes $35,000 a year — or more — doesn’t get a dime in Obamacare subsidies. She’s too young and too middle class.
Under the 2017 Project’s alternative, every 40-year-old single woman would get a $2,100 tax credit, to help her buy health insurance of her choice.
Even though it would benefit far more people than Obamacare, such an alternative would actually cost much less — which is a testament to how expensive Obamacare is and how lavish its subsidies are for the chosen few. According to the nonpartisan Center for Health and Economy, which is co-chaired by Princeton health policy expert Uwe Reinhardt and former CBO director Douglas Holtz-Eakin, the 2017 Project’s “Winning Alternative to Obamacare” would save $1.1 trillion in federal spending over a decade versus Obamacare, while increasing the number of people with private health insurance by 6 million versus Obamacare. It would also substantially lower premiums and dramatically expand access to doctors. It would provide the sort of real reform Americans want.
The 2017 Project’s alternative would also provide commonsense consumer protections, as well as funding for state-run “high risk” pools, to ensure that no one could be denied affordable health insurance on the basis of a preexisting condition. For example, no one could be dropped from his or her existing insurance, or be re-priced, due to a health condition. When young men or women turn 18, or leave school and go off of their parents’ insurance, they would have a one-year buy-in-period during which they could not be denied coverage, or charged more, for a preexisting condition. Parents would have a similar one-year buy-in-period for newborns. People could move from employer-based plans to individual plans, or move from one individual plan to a similar or cheaper individual plan, without being denied coverage or being re-priced because of a preexisting condition. And $7.5 billion a year in federal funding for state-run high-risk pools would ensure that anyone could buy partially subsidized insurance, through these pools, that covers preexisting conditions.
If Congress were to give states an off-ramp that leads to simple, flat, age-based tax credits for everyone in the individual market, protections for those with preexisting conditions, and the elimination of all of Obamacare’s liberty-sapping mandates, it would be a very popular proposal.
The millions of mostly lower-income Americans who had been getting Obamacare subsidies in defiance of the law’s plain language — and who would be getting nothing in the wake of a ruling against the administration — would get a generous tax credit to help them buy affordable insurance of their choice. Moreover, because they were already covered, if they were to switch to a more affordable plan, they could not be charged more — or denied coverage — because of a preexisting condition.
Meanwhile, the millions — perhaps tens of millions — of middle-class Americans who have never gotten anything under Obamacare would get a long-overdue tax break to buy insurance of their choice. Such tax breaks would be worth thousands of dollars to millions of Americans. They would finally fix what the federal government has broken through the tax code and allow the individual market to flourish.
States deserve an off-ramp from Obamacare that leads to a winning alternative. For six years, Americans have opposed Obamacare and have waited to be offered something better. Now is the time to give it to them.
(The 2017 Project’s full proposal, entitled “A Winning Alternative to Obamacare,” follows.
A Winning Alternative to Obamacare
Introduction
Obamacare was passed as “comprehensive” legislation, and it calls out for comprehensive repeal. But even though the American people detest Obamacare, they won’t support its comprehensive repeal if that means going back to the pre-Obamacare status quo. While most Americans would personally like to see Obamacare repealed, they are not likely to yank newly obtained insurance away from millions of their fellow citizens. It is therefore crucial for conservatives to advance a winning alternative that alleviates this concern and leads to Obamacare’s ultimate defeat.
There are three reasons why advancing an alternative is so important: (1) politically, one cannot expect to beat something with nothing; (2) policy-wise, our health-care system already needed to be fixed pre-Obamacare, because the federal government had already broken it; and (3) if Obamacare continues to unravel but conservatives offer no viable alternative, liberals will seize the opening to push for the government monopoly over American medicine (“single payer”) they have always desired.
The common formulation is that we need to “repeal and replace” Obamacare. The truth is more nearly the reverse: We need to advance a winning alternative to pave the way to full repeal.
A well-conceived conservative alternative would be able to make the following winning claim: Under the conservative plan, health costs would drop, liberty would be secured, and any American who wants to buy health insurance would be able to do so.
Before Obamacare, Americans had three core concerns with our health-care system, and a victorious alternative needs to offer compelling solutions to all three: the large number of people without insurance; the no-man’s-land plight of those who are uninsured and have expensive pre-existing conditions; and the high cost of care. To a large extent, the solution to all three problems involves fixing what the federal government had already broken even before liberal politicians defied public opinion and rammed Obamacare into law, making things far worse. As such, real reform requires shifting things in a conservative direction from the pre-Obamacare status quo.
In the absence of such a conservative alternative, President Obama’s signature legislation will survive. But a well-conceived alternative would lead to Obamacare’s complete undoing and unconditional defeat, to the great benefit of the American people.
To invoke the second-greatest Republican president, now is a time for choosing. Conservatives can advance a winning alternative to Obamacare and thereby strike a historic blow for limited government and liberty. Or else—whether because any alternative won’t be quite what they might have chosen in a political vacuum, because of political miscalculations, or simply because of inertia—they can watch Obamacare, or whatever it spawns, become cemented on these shores.
A Proposed Alternative
Whatever an alternative’s exact features, there are three elements that are important, and perhaps essential, to its being a political and policy winner—and thus to its being instrumental in bringing about Obamacare’s full repeal. First, a winning alternative must be something that can be sold to the American people on the political stump. It must therefore be suitably simple and explainable. Second, it cannot afford to invite a political backlash by proposing ideas that are lightning rods for criticism. For example, it shouldn’t veer into important but nevertheless tangential issues like Medicare reform, and it shouldn’t threaten the existence of the tax break for those with employer-provided health insurance (although it can—and should—prevent that tax break from being an open-ended public subsidy for ever-more-expensive plans). Third, and most importantly, it must meaningfully address Americans’ trio of core goals for real health-care reform: lowering costs, dealing with preexisting conditions, and significantly increasing the number of people who are insured versus the pre-Obamacare status quo. Indeed, failing to offer solutions to each of these concerns is the easiest way for a conservative alternative to become a target for criticism. An alternative that meaningfully addresses only two of these three core goals would be toppled over like a two-legged stool.
In that spirit, we present the following “three legged” proposal, which borrows extensively from ideas advanced by a wide array of conservative commentators and policymakers, as an alternative to Obamacare’s 2,700 pages of unprecedented federal largess.
The First Leg: Ending the Unfairness in the Tax Code—by Offering Tax Credits to the Uninsured and Individually Insured
The core of any winning alternative must be its ability to provide a solution to the longstanding problem of too few people having health insurance. Fortunately, such a solution mostly involves fixing what the federal government had already broken pre-Obamacare. For decades, the federal government has had its foot on the scale, favoring employer-provided health insurance by giving it preferential treatment in the tax code. Why should millions of Americans who get insurance through their employer get a tax break, while millions who buy it on their own through the individual market, do not? This is unfair, and it makes no sense.
What’s more, this is a place where a conservative alternative would prove very popular, because it would solve a problem that Obamacare—despite its extraordinary expense and brazen recourse to government coercion—has failed to solve. In addition to the myriad ways in which Obamacare undermines our liberty and our health-care system, it fails to equalize the tax treatment of health insurance. (Indeed, in the case of the self-employed—who used to get a tax break for buying health insurance but now don’t—it has made the problem worse.)
Obamacare provides massive taxpayer-funded subsidies to older Americans at the expense of younger ones, and to the near-poor at the expense of the middle class. But it provides no subsidies and no tax breaks in the individual market to most single people in their 20s or 30s who make over $35,000 a year, none to most single people under 50 who make over $40,000 a year, and (thanks to its marriage penalty) none to any married couples without children who make over $65,000 a year (see the 2017 Project’s Study on Obamacare’s Subsidies and Penalties, specifically “Median Obamacare Subsidies by Age and Income”). All of those solidly middle-class Americans continue to have to pay federal taxes on their income and then use a portion of what’s left to buy health insurance, while millions of their fellow Americans get to have their health insurance provided with tax-free income, simply because they get it through their employer.
In a political vacuum, one might consider addressing this unfairness in the tax code by ending and replacing the tax break for employer-provided health insurance. But as James Capretta, Tom Miller, Ramesh Ponnuru, Yuval Levin, and others have noted, this would be politically foolish and would badly undermine efforts to repeal Obamacare. If that weren’t already clear beforehand, the experience of lost plans under Obamacare has surely made it plain. The American people do not want anyone messing with their existing insurance.
Rather than ending the employer-provided tax break, the sensible solution, then, is to offer a corresponding tax break in the individual market, thereby more or less leveling the playing field. To avoid suffering a tremendous decline in the number of people who have insurance (versus the number of insured under Obamacare), such a tax break needs to take the form of a tax credit. This is the approach that Senator Jim DeMint wisely advocated as far back as 2009, and that Senators Tom Coburn, Richard Burr, and Orrin Hatch have more recently advanced.
We propose providing a refundable health insurance tax credit of $1,200 for those under 35 years of age, $2,100 for those between 35 and 50 years of age, and $3,000 for those over 50, in addition to $900 per child. These tax credits would be made available to those, and only to those, who purchase health insurance through the individual market.
The value of the credits would rise 3 percent per year. That is less than the historical rate of health-care inflation, but the point of these credits is to revitalize an individual market that the federal government has broken, thereby lowering health costs. Besides, Congress can always raise such spending, but it is better to require an affirmative vote for such a change than to put such spending increases on excessively generous autopilot, as has too often been done before.
Every American citizen or family who is looking to buy insurance through the individual market would be able to use such a tax credit to help buy an insurance policy of their own choosing. There would be no more Obamacare decrees forcing everyone to buy insurance that covers such things as maternity care, pediatric dental care, or the abortion drug ella, and no more corralling of free citizens into government-run exchanges. Moreover, the tax credit would go directly to individuals or families, not to insurance companies like the Obamacare subsidies do.
The vast majority of Americans shopping in the individual market would supplement this tax credit with their own expenditures, freely choosing to buy insurance that costs more than the tax credit would cover. For them, the tax credit would be a source of savings, freeing them from the burden of paying for all of their insurance costs with after-tax dollars, while those with employer-based insurance have theirs paid for with pre-tax dollars. For example, for a family of four with parents in their early 30s, the tax credit would cover the first $4,200 in premiums ($1200 x 2 + $900 x 2), and they could, of course, supplement that with whatever amount they choose. Meanwhile, those who buy insurance that costs less than the amount of the tax credit would be allowed to keep the difference and put it into a health savings account (HSA).
Even those who didn’t contribute a dime of their own money would still be able to use the credit to buy basic coverage providing protection against a potentially catastrophic illness. Indeed, tax credits of these amounts would make it possible for people in most of the 50 states who choose to buy health insurance, to buy it—based on a report on individual-market insurance premiums published by the Government Accountability Office. The exception would be those living in one of a handful of extremely liberal states, where hyper-regulation has caused insurance prices to skyrocket.
That GAO report examined individual-market premiums in all 50 states for a 30-year-old single man, a 30-year-old single woman, a 40-year-old couple with two children, and a 55-year-old couple without children. It reflected premiums in 2013 and therefore took into account the massive premium spike in 2011, when, in the wake of Obamacare’s passage the previous year, premiums went up 9.5 percent across all markets combined, according to the Kaiser Family Foundation—roughly twice the average annual premium increase over the previous five years.
The GAO report showed the following: Using the tax credits recommended in this proposal, members of all four examined demographic groups could have purchased insurance through the individual market in any of the 50 states, either just by using the tax credit or else by supplementing it with no more than $15 a month of their own money—except in the liberal havens of Maine, Massachusetts, New Jersey, New York, or Rhode Island. (Some smokers would also have had to pay a bit more to cover premiums in Alaska, Washington, and Wyoming.)
Even people in those five liberal states, however, would be able to buy insurance using just the tax credits under this proposal, as we would let them buy affordable insurance across state lines (see Part 3: Lowering Health Costs).
Contrast this $15-a-month-or-less cost with Obamacare. Under Obamacare, the typical person who makes $40,000 a year cannot get health insurance for ten times that price. That bears repeating: he or she cannot get health insurance for ten times that price. According to a 2017 Project study that examined the 50 largest counties in the United States, the median amount that a 26-year-old who makes $40,000 has to pay per month for Obamacare’s cheapest “bronze” (lowest tier) plan is $159. (Despite Obamacare’s extravagant cost, such a person isn’t eligible for a taxpayer-funded subsidy—being too young and too middle class.) At that same $40,000 level of income, the typical 36-year-old has to pay $191 a month, the typical 46-year-old has to pay $202 a month, and the typical 56-year-old—the only person on this list who gets a taxpayer-funded subsidy—has to pay $193 a month (post-subsidy).
In each instance, that’s a far cry from paying no more than $15 a month—a ten-fold difference. For the typical American shopping in the individual market, there would be no comparison between how affordable health insurance would be under this proposal and under Obamacare.
* * *
In all, a tax credit to buy health insurance through the individual market would offer myriad benefits. It would end the unfairness in the tax code, grease the wheels for Obamacare’s repeal, open up access to affordable coverage, fuel competition among insurers, breathe new life into a moribund individual market, and greatly increase the number of people with insurance versus the pre-Obamacare status quo at just a fraction of Obamacare’s cost. Moreover, because the credit wouldn’t remotely cover the cost of the lavish prepaid health plans that aren’t really (merely) insurance, it would also encourage the purchase of genuine insurance that protects against unforeseeable costs, while putting people in control of their own day-to-day health-care dollars. This would provide more people with the opportunity and incentive to shop for value, which in turn would cause providers to show prices as they compete to attract value-conscious customers. The result would be significantly lower health costs.
Ending the unfairness in the tax code by offering a refundable tax credit for the purchase of insurance through the individual market is the core element of a well-conceived alternative. Indeed, this first leg is the most important of the three legs that any winning alternative to Obamacare must feature—and, with it in place, Obamacare would be poised to fall.
Question & Answer: Who would receive a tax credit to purchase health insurance?
In addition to those currently buying (or looking to buy) insurance through the individual market, the tax credit would be made available to those who currently get insurance through a relatively small employer. If employees of such small businesses choose to buy insurance in the individual market, rather than getting their insurance through their employer, they would be free to do so—and thus to claim the individual-market credit. Those who work for larger employers and get insurance through them would continue doing so (so long as their employer continues to offer it), thereby protecting those employees’ employer-provided coverage while also protecting their employers from a selective exodus into the individual market by their healthier employees, which would lead to higher costs for those who remained behind.
In addition, the tax credit would be available to anyone who is eligible for Medicaid but who would prefer to receive the credit and purchase private health insurance.
The only (very minimal) requirement, in all cases, would be that the credit be used to purchase real insurance—namely, insurance that is licensed and solvent, that has very high or nonexistent annual and lifetime caps on coverage, and that frees the enrollee of any cost-sharing obligation past a certain point (by declaring the enrollee’s maximum out-of-pocket expenditure).
No one would be auto-enrolled in any insurance plan. And the credit would be received only by those who purchase insurance, not by those who don’t.
Q & A: Why offer a tax credit rather than a tax deduction?
Obamacare is perhaps the worst piece of legislation in American history. The central purpose of any conservative alternative, therefore, must be to pave the way to its full repeal. The key to achieving this result is to meet Americans’ trio of core goals for real health-care reform: substantially increasing the number of people who are insured versus the pre-Obamacare status quo; solving the problem of prohibitively expensive preexisting conditions; and lowering health costs. A tax deduction cannot effectively meet the first of these three key goals, so an alternative that centers around a tax deduction would struggle to pave the way to full repeal.
The vast majority of the benefits from an income-tax deduction would go to the top half of income-earners (as the New York Times would be quick to point out). As is well known by now, a significant portion of Americans don’t pay any income taxes, so an income-tax deduction would have no effect whatsoever on such Americans’ income-tax burden. A deduction that also applies to payroll taxes would benefit all workers, but it would also further reduce the number of Americans who don’t pay any federal taxes whatsoever (whereas a tax credit would leave payroll taxes alone). At the same time, a deduction that includes payroll taxes would likely still fail to meet the goal of substantially increasing the number of people who are insured versus the pre-Obamacare status quo.
A specific example might help illustrate the difficulty of relying on a tax deduction in this regard. Even a very large tax deduction of, say, $10,000 for an individual, which applies to both income and payroll taxes—and which applies in full regardless of whether someone spends anywhere near that much on health insurance—would still net a tax break of only $765 for someone who pays only payroll taxes (a pittance compared to Obamacare’s lavish taxpayer-funded subsidies for the near-poor, which are slated to grow more lavish over time). At the same time, it would provide a tax break of over $3,200 for millions of Americans in the upper half of the income stratum.
For an alternative to be able to make the winning claim that, under its provisions, any American who wants to buy health insurance would be able to do so, a tax credit—not a deduction—must be a centerpiece of the proposal. Whatever understandable theoretical misgivings some might have about refundable tax credits, supporting one in this context is a small price to pay to take down Obamacare.
Q & A: Why not means-test the tax credits?
Most of these tax credits will take the form of a tax cut for the uninsured and individually insured. But the portions that don’t—because the credits’ recipients don’t pay as much money in income taxes as they will get through the credits—will count as spending. Most of that spending—more than two-thirds, in fact—will be paid for by the top ten percent of income-earners. Not making the credit available to people at that income level would therefore be like having ten people order dinner together in a restaurant, having one of them pick up two-thirds of the tab, and then telling that person that he or she can’t have any of the food.
The credits would already be quite progressive in their impact: the wealthier would cover most of the cost of them, while the less-wealthy would receive most of the benefits from them. Yet there is also a level of equality, fairness, and simplicity involved: each person would get the same credit, subject only to his or her age (a factor that directly relates to health costs). To make the program available to all but, say, the top 10 percent of income-earners would shift it from being a program for all Americans to being something more akin to a welfare program for the middle class.
Additionally (and importantly), the goal here—apart from paving the way to full repeal—is to end the unfairness in the tax code. Wealthier Americans already get a tax break for employer-provided health insurance and will continue to get one. (Under this proposal, however, that tax break would no longer be open-ended and wouldn’t offer ever-higher tax-breaks for ever-pricier plans.) To deny wealthier Americans a tax break in the individual market, therefore, would not only be unfair but would artificially incentivize them to seek insurance through an employer (if at all possible), rather than through the individual market.
Many conservatives believe that Medicare should be means-tested, but these two positions (espousing means-testing for Medicare and opposing means-testing for these tax credits) are mutually consistent. Medicare is a huge, liberal-designed program whose runaway costs are careening us toward bankruptcy and whose financing offers no pretense of involving anything other than a massive redistribution of wealth (unlike Social Security, whose financing is at least based on the general principle, however imperfectly applied, of paying in for oneself).
What’s more, there is an important difference between fixing a broken program (like Medicare) and designing a new one (as an alternative to another liberal-created monstrosity—Obamacare). A program of conservative design should reflect conservative principles. One of Obamacare’s worst features is its obsession with income, which pits Americans against one another and empowers the federal government to redistribute money from young to old and from the middle class to the near-poor (leaving a good chunk of cash behind in Washington, D.C., of course). The conservative alternative shouldn’t focus on income but should instead embrace simplicity and treat all Americans equally. It’s quite enough that the top ten percent of income-earners will have to pay for most of the cost of the tax credits. They don’t also need to be denied their benefits.
Q & A: How much would this cost, and how would it affect the middle class?
Obamacare’s taxpayer-funded subsidies and its Medicaid expansion are poised to cost over $2 trillion from 2015 to 2024, according to the CBO (see Table B-1). The CBO says that over 90 percent of that amount—$1.863 trillion (assuming the same rate of growth from 2023 to 2024 as from 2022 to 2023)—would come in the form of direct spending (new outlays).
This alternative, meanwhile, is estimated to cost only $977 billion—and most of that “cost” (that’s how the CBO would label it) would come in the form of a tax cut. It would save taxpayers more than $1 trillion versus Obamacare from 2015 to 2024—with the annual savings increasing each year, as the following chart shows:
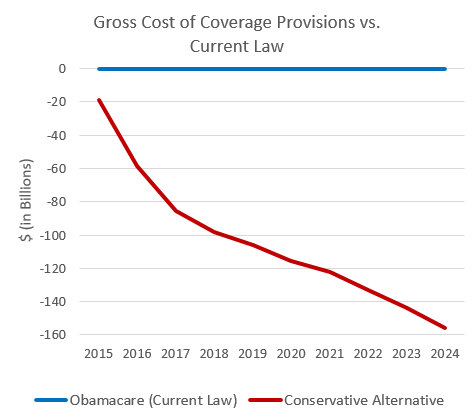
Moreover, in terms of direct spending, this alternative is estimated to cost only $399 billion over a decade—less than a quarter as much as Obamacare—a savings of $1.464 trillion.
It is therefore amazing that—even apart from this alternative’s beneficial effects on their liberty, their health care, and their role as taxpayers—the vast majority of Americans would personally fare much better under this proposal than under Obamacare, as the following chart demonstrates:
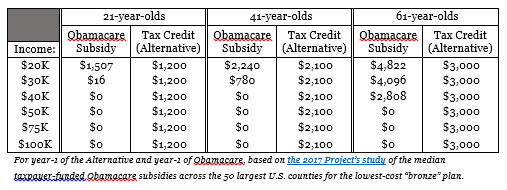
How, in light of this chart, can Obamacare be so expensive? First, its outlays for its Medicaid expansion—a part of Obamacare that President Obama rarely emphasizes—are huge, making up 43 percent of Obamacare’s direct spending over the next decade, according to the CBO. In fact, in terms of direct spending, Obamacare’s Medicaid expansion alone is poised to cost more than this entire alternative. Second, the taxpayer-funded subsidies for Obamacare’s exchange plans are projected to skyrocket in future years in response to the premium spikes that the health-care overhaul is causing. The CBO projects (see Table B-1) that Obamacare’s taxpayer-funded premium and cost-sharing subsidies will cost a hefty $20 billion in 2014 but a whopping $159 billion in 2024—nearly an eight-fold increase in just ten years. Third, Obamacare’s subsidies, not only for premiums but also for the out-of-pocket costs of care (copays, deductibles, etc.—95 percent of which would be covered by taxpayers in some cases) are massive for those who make under $20,000 and those who make under $30,000 and are over 60 years of age—as Obamacare redistributes huge amounts of wealth from younger to older Americans and from the middle class to the near-poor. Thus, its benefits are narrowly distributed, while its costs are widely felt. With the right alternative on the table, that’s a recipe for political defeat.
Q & A: How would this be paid for?
As noted above, the tax credits proposed through this alternative would largely take the form of a tax cut for the uninsured and the individually insured. But the portions that wouldn’t—because the credits’ recipients don’t pay as much in income taxes as they would get through the credits—would count as spending. That spending, an estimated $390 billion from 2015 to 2024, would be more than offset by the estimated $679 billion in increased revenue that would result from closing the tax loophole that currently provides an open-ended public subsidy for ever-more-expensive employer-based plans (see Part 3). Meanwhile, an estimated $86 billion in funding for “high risk” pools (see Part 2) would be mostly offset by an estimated $77 billion reduction in Medicaid spending versus the pre-Obamacare status quo, resulting from some Medicaid beneficiaries freely choosing to use tax credits to buy private insurance in lieu of staying on Medicaid. After factoring in the remaining “cost” of the tax credits ($578 billion), a shortfall of $298 billion would remain—but it’s a shortfall that would result from a tax cut. This could be paid for in a variety of ways, including by reducing all non-defense spending—across all federal departments and agencies—by just three-quarters of 1 percent (0.75 percent) from 2015 to 2024.
That certainly compares favorably to the funding for Obamacare, which (according to CBO figures) involves cutting Medicare spending by about 12 percent from 2015 to 2024 and using that money to pay for Obamacare (even as the Obama administration disingenuously claims that it’s somehow also using that same money to extend the life of Medicare) and raising taxes by more than $1 trillion over that same 10-year span.
Q & A: Is this Obamacare Lite?
If not repealed, Obamacare will increase direct federal spending by the better part of $2 trillion over the next decade (2015 to 2024), even though we’re already more than $17 trillion in debt. Over that same span, it will funnel nearly $1 trillion from taxpayers, through Washington, to insurance companies. It will siphon nearly $1 trillion out of Medicare, to be spent on Obamacare. It will cut Medicare reimbursement rates to the point where Medicare providers will be paid less than Medicaid providers by the end of this decade. It will establish the unelected 15-member Independent Payment Advisory Board, whose largely unaccountable decrees won’t be reversible even by a simple majority of the House and Senate and the signature of the president. It will provide taxpayer funding of abortion. It is already causing millions of Americans to lose their health plans and their doctors. It is causing health insurance premiums to soar. It is causing many if not most of the newly insured to be dumped into the broken Medicaid system at taxpayer expense. It is causing employers to dump their employees into Obamacare’s exchanges at taxpayer expense. It is forcing the young to help pay the bills of those who are older and generally more affluent. It is exacerbating a looming doctor shortage. It is providing huge disincentives for businesses to hire new workers, which is a large part of why this “recovery” still looks a lot like a recession. It is mandating—in a way that the federal government has never done before—that private American citizens must buy a product of the federal government’s choosing merely as a condition of living in the United States.
This alternative would do none of those things.
Instead, it would pave the way to Obamacare’s full repeal, wipe the slate clean, and then implement real health-care reform that shifts things to the right of the pre-Obamacare status quo.
Here’s what Obamacare Lite looks like: Conservatives fail to advance a winning alternative, and Obamacare isn’t repealed but is merely “tweaked,” “improved,” or “fixed.” Its basic structure remains the same—built according to its 2,700-page, Constitution-defying blueprint—but portions of it are made somewhat less objectionable at the margins. In all, Obamacare generally survives, becoming perhaps 80 percent as bad as it once was. In other words, it becomes what it would have been from the start had Obama not so arrogantly refused to work with a handful or two of overly accommodating Republican senators back in 2009—a foolish rejection of bipartisanship that left the door wide open for the full repeal of his resulting monstrosity. But Obama’s greatest political blunder never comes back to haunt him, as conservatives refuse to offer up the alternative that would lead to full repeal. As a result, power and money are consolidated in the nation’s capital to a heretofore unprecedented degree—at great loss to American medicine, Americans’ liberty, and America’s fiscal solvency.
The Second Leg: Solving the Problem of Expensive Preexisting Conditions
Predictably, Obamacare’s use of heavy-handed coercion in dealing with preexisting conditions has caused health insurance premiums to skyrocket. In order to expand insurance coverage to those who are already sick, Obamacare bans insurers from basing the price of a policy on the health status of an applicant. In doing so, it encourages people to game the system by waiting until they get sick or injured before purchasing insurance, which is a lot like letting people buy homeowners’ insurance after the fire trucks have already arrived on the scene.
Fortunately, there are ways to meet this same goal that don’t send insurance costs soaring and don’t uproot the very notion of what insurance is. In that spirit, we offer the following six-part proposal:
First, we propose that no one be able to be dropped from their existing health insurance plan, or have their premiums or other costs increased, on the basis of a health condition. This protection would apply both to health conditions that developed after a policy took effect and to ones that were already in existence when a policy took effect and were not willfully hidden from the insurer. This protection would apply to all plans, including those purchased during the unfortunate Obamacare era. This alternative—very much unlike Obamacare—wouldn’t cause people to lose the health insurance they already have.
Second, we propose a one-year buy-in-period for young adults who are looking to buy health insurance on their own for the first time, during which time they would be exempted from paying more or being treated differently due to preexisting conditions. This one-year buy-in-period would start on a person’s 18th birthday. For those who remain covered under their parents’ health insurance (perhaps because they are full-time students), this one-year grace-period would begin once they cease to be covered under their parents’ insurance, or on their 25th birthday—whichever comes first. With this framework in place, no responsible young person would face higher health insurance costs simply because he or she happens to suffer from an inborn medical condition or a condition that was acquired as a child.
Third, we propose that parents be granted a similar one-year buy-in-period for newborns, during which time they couldn’t be denied insurance for their child, or be charged more, because the child was born with, or had quickly acquired, a preexisting condition. And once insured, the child couldn’t be charged more for that condition going forward, either under that plan (per our first proposal in this section) or under a different plan at that same level of coverage (see the fifth proposal, below).
Fourth, we propose easing the transition from employer-based insurance to the individual market in the following manner: Those who have maintained continuous employer-sponsored coverage (for a period of at least a year), but then lose access to that coverage, should be able to transition to a plan in the individual market—one of their own choosing—without paying higher premiums because of a preexisting condition. We would allow a two-month grace-period between the time that someone leaves a job (or otherwise loses access to an employer-provided plan) and the time that he or she buys insurance through the individual market, during which time those protections would apply.
Fifth, drawing upon the work of health policy experts such as James Capretta and Tom Miller, we propose new regulations to protect Americans if they stay continuously insured and want to switch from one individual-market plan to another. Under these regulations, those who have remained continuously insured in the individual market (again, for at least a year) could switch to a different plan—either with their existing insurer or another—that provides the same level of coverage (with such classifications to be determined by the states), without paying more because of a preexisting condition that has developed since they first became insured under their current plan.
Sixth, we propose allocating $7.5 billion a year (with a 3 percent annual increase following year-1) in federal funding for state-run “high risk” pools, an insurance framework championed by Capretta, Miller, and others. Those with expensive preexisting conditions would be able to purchase policies through state-run, federally subsidized high-risk pools. Through such high-risk pools, a person could purchase a partially subsidized health insurance policy, and his or her share of the premiums could not exceed some set percentage (say, 150, 200, or 250 percent)—with the exact percentage to be set by each separate state—of the average cost of a policy for a person without preexisting conditions in that same demographic group (based on age, sex, and geography). No one could be denied coverage through such high-risk pooling, no matter how unhealthy he or she might be.
Crucially, this federal funding would be provided to each state as a defined contribution. Each state would get a set amount each year (to spend only on its intended purpose) based upon its population of American citizens. While most states would likely supplement this federal funding with funding of their own, states’ outlays would not trigger any matching federal funds. As Medicaid and other examples have sufficiently demonstrated, the practice of matching states’ contributions with federal money merely encourages states to be generous in spending money (as every dollar spent nets them more in federal revenues) and reluctant to stop spending money (as every dollar cut nets them only some portion of that in savings).
In combination, these six provisions would ensure that no one in America would be denied affordable health insurance on the basis of an expensive preexisting condition.
The Third Leg: Lowering Health Costs Across the Board
It would be hard not to lower health costs in relation to Obamacare, and the American people know it. Indeed, even before liberals wilfully passed President Obama’s signature legislation into law, the CBO projected that, by 2016, Obamacare would cause the average health insurance premium in the individual market to be 10 to 13 percent higher, per person, than it otherwise would have been. Earlier that same month, the CBO had projected that the 2009 House Republican health-care bill would cause the average health insurance premium in the individual market to be 5 to 8 percent lower, per person, than it otherwise would have been. That’s a 15 to 21-point swing in premiums between the House GOP proposal and Obamacare.
For families, the projections for Obamacare were even worse. The CBO projected that, by that same year, Obamacare would cause the average family’s premium in the individual market to be 16 percent—and $2,100—higher than it otherwise would have been. Adding in the CBO’s projected savings on the Republican side ($655 at 5 percent, $1,048 at 8 percent), the average American family’s health insurance premium would have been about $3,000 a year lower under the Republican plan than under Obamacare. For the typical American family, that’s a lot of money.
To be sure, that’s before factoring in Obamacare’s expensive taxpayer-funded subsidies. However, the typical middle-class American would fare much better under the tax credits proposed in this alternative than under the Obamacare subsidies—as those subsidies aren’t remotely geared toward the middle class (see the chart in Part 1).
The key to lowering health costs is to inject new life into the individual market, which has long labored under a huge government-created disadvantage. The tax credits proposed herein would have the effect of taking the government’s foot off the scale, more or less equalizing the tax treatment of individual and employer-based plans, and the individual market would flourish as a result. In addition, however, we propose borrowing from the 2009 House Republican bill, from the Republican Study Committee’s recently released America Health Care Reform Act, and from the Coburn-Burr-Hatch proposal, all of which would liberalize rules regarding contributions to, and spending from, health savings accounts (HSAs).
To further encourage the use of HSAs, and to help people cover the day-to-day costs of care, we additionally propose a one-time tax credit of $1,000 per person to anyone who opens an HSA for the first time in the individual market, as well as to anyone who has already opened an HSA in the individual market but has never claimed this credit. (The credit would continue to be offered in subsequent years, but no person could claim it more than once, and its value would not increase over time.) The credit would be deposited directly into an HSA, and the result would be that anyone in America who opens an HSA would effectively start with $1,000 in it (or $2,000 for a couple, or $4,000 for a family of four). At relatively minimal cost (since it’s a one-time credit, per person), this would incentivize the use of HSAs, which encourage people to take control of their own health-care dollars and allow them to spend those dollars tax-free. It would also help to rebut the inevitable criticism from the left that some people cannot afford to cover the out-of-pocket cost of any of their care. In these ways, such a one-time tax credit would complement the tax credit for purchasing health insurance on the open market.
We also propose lowering costs by having Congress free up the interstate purchase of health insurance. There is no good reason why a couple in New Jersey, for example, should be prevented from purchasing a health insurance plan that originates in Texas and meets Texas’s rules (rather than New Jersey’s) regarding what things the policy must cover, any limitations on pricing, etc. As such, our alternative would replicate proposals introduced by Sen. Jim DeMint, Rep. Tom Price, and the Republican Study Committee (among others), by allowing people to shop for and purchase health insurance across state lines.
While encouraging people to maintain more control of their own health-care dollars and giving them more opportunity to shop for value, it is also important that a winning conservative alternative move away from the open-ended subsidizing of health insurance that undermines such cost-consciousness. Thus, we propose capping the now-limitless deduction for employer-sponsored health insurance. To be clear, every employer-based plan would continue to get a tax break. But in place of the open-ended deduction for employer-sponsored insurance, we propose capping the maximum deduction at the 75th percentile of employer-sponsored plans, in terms of the cost of their premiums (so, at a level where only the 25 percent of employer-based plans that are the most expensive would be affected at all), and having that amount rise 3 percent annually from there. The CBO projects that, in 2015, the only insurance plans that would be affected by this provision would be those that cost roughly $8,000 per individual or $20,000 per family (see p. 247). If a family plan costs, say, $22,000 and the cap is set at $20,000, a family with that plan would continue to get a tax break on the first $20,000 of its cost; it simply wouldn’t get a tax break on the last $2,000.
Closing this tax loophole, which incentivizes people to spend more on health insurance than they would if it weren’t tax-free, would not only help equalize the tax treatment of employer-sponsored and individual-market insurance—while offsetting most of the revenue loss from the tax credit—but it would also help lower health costs. In the example provided above, the family in question might decide to buy a plan that’s $2,000 less expensive and spend that extra $2,000 on something else, and their slightly cheaper insurance plan—being a bit less like prepaid health care and bit more like genuine insurance that protects against unforeseen costs—would likely give them a bit more opportunity and incentive to shop for value. And the more people are shopping for value (and not just have their expenses covered by a middleman), the more health costs will come down across the board.
We also propose letting people reap the rewards if their lifestyles minimize their risk of needing costly care. Obamacare gives insurers no leeway to reward such healthy behavior and in fact bans them from doing so. But as Rep. Paul Ryan, Sen. Tom Coburn, Sen. Richard Burr, and Rep. Devin Nunes noted in their 2010 bill, the Patient’s Choice Act, “five preventable chronic conditions consume 75 percent of our health spending and cause two-thirds of American deaths.” The 2009 House conservative bill would have allowed health insurers to vary the price of premiums by as much as 50 percent, contingent upon the policyholder’s participation in a wellness program. We would allow insurers to go even further, by removing any provision that keeps insurers from encouraging healthier lifestyles and from pricing policies accordingly.
Yet another contributor to high health costs that Obamacare ignores is frivolous medical malpractice lawsuits. Doctors seeking to protect themselves from legal action often feel compelled to assign extra tests or treatments, which inconvenience patients and greatly increase premiums and out-of-pocket costs. According to a survey of doctors conducted by Jackson Healthcare and Gallup, a staggering one-quarter of all health-care spending is a product of defensive medicine, totaling some $650 to $850 billion annually.
To reduce such wasteful spending, states should implement creative policies that will cut back on the number of frivolous medical malpractice suits and expedite the resolution of credible suits. States should consider capping noneconomic damages in medical malpractice suits at $250,000. Moreover, medical malpractice tribunals would likely offer a more efficient and affordable framework for resolving such suits. These tribunals could replace a traditional 12-man jury with a smaller panel of medical experts, who could decide on the merits of the suit and award damages accordingly.
The combination of these provisions would lower health costs substantially in relation to the pre-Obamacare status quo—and all the more in relation to Obamacare.
Conclusion
This “three legged” proposal is as intelligibly simple as Obamacare is unintelligibly complex. If conservatives were to advance something along these lines, Americans would get it, and they would embrace it. The vast majority of Americans, and particularly younger Americans and the middle class, would come out far better under this proposal than under Obamacare, even before factoring in how much they would save in taxes—or gain in liberty.